Peptides carry real risks. This guide covers the five primary safety concerns, how to verify quality, what baseline screening looks like, and when to stop.
TL;DR
Peptides are powerful compounds with real risks: immunogenicity, tissue toxicity, cardiovascular effects, contamination, and systemic organ damage can all occur. Safety depends on three non-negotiable steps: (1) verify quality via third-party CoA validation, (2) screen yourself medically before first injection, (3) follow a conservative dosing protocol with daily logging and monthly labs.
Medical supervision is mandatory for peptides with systemic effects. Contamination is widespread-a 2023 analysis found 100% of non-pharmaceutical peptides tested were contaminated; 26% exceeded safe limits for heavy metals. Quality verification, baseline screening, and monitoring separate safe use from reckless guessing.
Why Peptide Safety Matters More Than You Think
The Reddit thread that went viral last month-someone claiming their CJC-1295 protocol “rebuilt” their aging joints-had 2,000 upvotes before anyone mentioned the immunogenicity risk or asked whether they’d had baseline labs. That’s the problem. Peptides occupy this weird space where marketing hype is everywhere, safety data is sparse, and the difference between “generally well-tolerated in mouse models” and “safe for human use” is treated like a minor detail.
But that difference kills people. A dosing error with synthetic GLP-1 agonists lands you in the ER. Melanotan II in someone with a family history of melanoma is cancer-tier risk. Contaminated peptides don’t just cause injection-site infections-heavy metal contamination can cause irreversible kidney damage.
This guide isn’t here to tell you peptides are bad. Liraglutide, teriparatide, and glucagon have decades of clinical data and are genuinely useful. But the research peptides circulating in the biohacking community? Those exist in a regulatory gray zone where quality is a guess, contamination is common, and adverse effects are underreported because people using them aren’t in clinical trials.
This is how to actually use peptides safely-with the verification, screening, and monitoring that separates informed risk from Russian roulette.
The Five Primary Safety Concerns
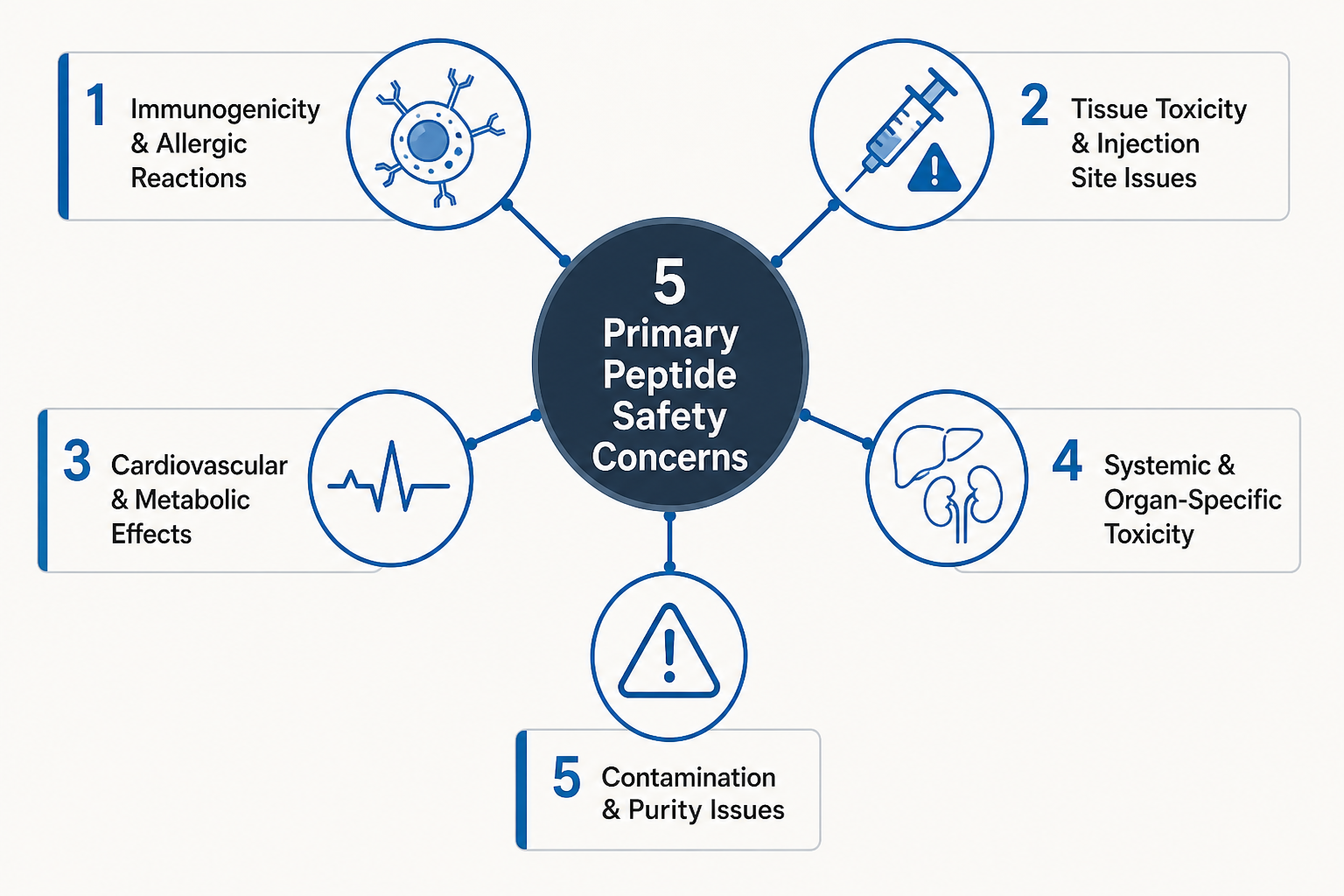
1. Immunogenicity & Allergic Reactions
Peptides are proteins. Your immune system recognizes foreign proteins. Sometimes it kills them silently. Sometimes it freaks out.
GHRH peptides (CJC-1295, ipamorelin, sermorelin) carry the highest immunogenicity risk. The growth-hormone-stimulating effect triggers a secondary cascade in some users-mast cell activation, histamine surges, localized or systemic allergic reactions.
What it looks like: Severe flushing within hours of injection, itching, urticaria (hives), angioedema (swelling of throat/face), anaphylaxis. The worst case is rare but documented.
Who’s at risk: People with baseline allergies, autoimmune conditions, or elevated mast cell activity (common in peri/menopausal women) have higher odds.
How to prevent it: Allergy testing before use. Start at 25% of planned dose for the first 2 weeks. Have antihistamines on hand. If anaphylaxis is a real concern, carry an EpiPen.
2. Tissue Toxicity & Injection Site Issues
A contaminated peptide, poor injection technique, or an improperly purified formulation can damage tissue. Lipohypertrophy, necrosis, sterile abscesses, and infections all happen when safety isn’t prioritized.
The critical distinction: Purity ≠ sterility. A 99% pure peptide can harbor bacterial spores or endotoxins that cause localized or systemic infection. Two separate tests.
How to prevent it: Use only autoclave-sterilized insulin needles. Rotate injection sites daily. Verify peptide sterility on the CoA (USP <71> or <797> certification). Use aseptic injection technique-alcohol swabs, clean hands, new needle every time.
3. Cardiovascular & Metabolic Effects
GLP-1 receptor agonists cause heart-rate elevation, blood-pressure changes, and nausea. In overdose, pancreatitis and hospitalization are documented. GHRH peptides can trigger arrhythmias in sensitive individuals. TB-500 (thymosin beta-4) has almost no human safety data; immune modulation effects are unknown.
How to prevent it: Baseline cardiovascular assessment (EKG if >40 or risk factors). Start low, go slow-titrate over 2–4 weeks. Monitor for palpitations or chest discomfort. Never combine GLP-1 with unprescribed insulin (severe hypoglycemia risk).
4. Systemic & Organ-Specific Toxicity
Kidney/liver stress, hormonal disruption, neurological effects. Melanotan II carries seizure risk in susceptible individuals. GHRH peptides affect cortisol and thyroid function-not always reversibly acute.
How to prevent it: Baseline organ-function tests (liver, kidney panels). Avoid mixing multiple peptide classes without medical oversight. Monitor thyroid function (TSH) if using GHRH peptides long-term.
5. Contamination & Purity Issues
Here’s where the real danger lives. A 2023 independent analysis found 100% of non-pharmaceutical peptide samples tested were contaminated; 26% exceeded safe limits for heavy metals (arsenic, lead, cadmium).
Why it happens: Unregulated manufacturing, poor quality control, intentional adulteration, cross-contamination. “Research grade” doesn’t mean safe. It means “not sold as a drug” and dodges FDA oversight.
How to prevent it: Demand third-party testing results independently verified. A good CoA includes purity %, identity confirmation, sterility, endotoxin limits, and heavy metals screening. Verify the testing lab directly-don’t trust vendor claims alone.
Quality Assurance: What a Real Certificate of Analysis Must Show
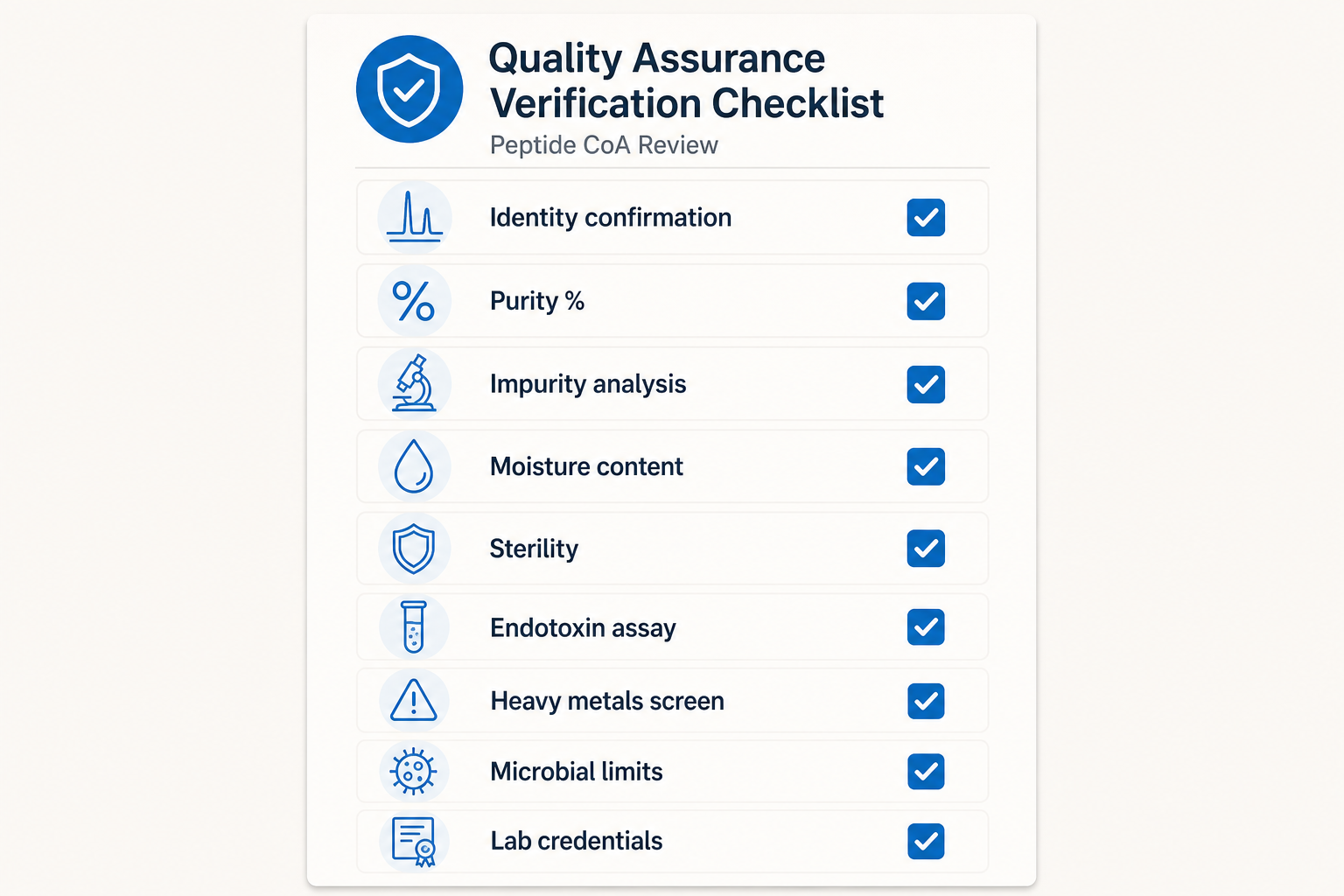
When you request a CoA, demand these nine elements:
- Identity confirmation – HPLC chromatogram + MS data showing the peptide’s molecular weight matches the claimed compound. Not guessing. Proof.
- Purity % – The percentage of actual active peptide. Acceptable ≥95% for research; ≥98% for anything you’re injecting. Single number only-if it says “major component >95%, other stuff <5%,” ask what the “other stuff” is.
- Impurity analysis – Specific impurities identified and quantified. Not just a total. If the CoA doesn’t name them, it’s hiding something.
- Moisture content – Must be ≤5% for peptide stability. Higher than that, and the peptide degrades faster.
- Sterility test – USP <71> (membrane filtration) or USP <797> (compounded) certification. No sterility test = don’t inject it.
- Endotoxin assay – LAL test result. Typical safe level is <10 EU/dose. High endotoxin causes fever, inflammation, and in severe cases, sepsis.
- Heavy metals screen – ICP-MS or ICP-OES for arsenic, lead, cadmium, mercury. Each should be <2 ppm. This is where contamination typically hides.
- Microbial limits – Total aerobic count, yeast/mold count (USP standards). Should match compendial limits.
- Test lab credentials – ISO 17025 certification. You should be able to contact the lab directly to verify results weren’t forged.
Red flags:
- Vendor refuses to provide CoA or claims it’s “confidential”
- CoA lacks sterility or heavy metals testing
- Prices unusually cheap (quality costs money)
- Lab can’t be verified independently
- Vague origin or supply chain
Green flags:
- CoA from accredited lab (ISO 17025)
- Vendor willing to re-test through independent lab
- Transparent supply chain
- Responsive to technical questions
- Peer reputation in research communities
Dosing, Screening, Monitoring: The Safety Protocol
Step 1: Medical Screening (Before First Injection)
Non-negotiable baseline labs:
- Blood glucose & HbA1c – Metabolic safety foundation. GLP-1 agonists are contraindicated in uncontrolled diabetes.
- Kidney function – Creatinine and BUN. GHRH peptides are renally cleared.
- Liver function – AST and ALT. Some peptides stress the liver at high doses.
- Lipid panel – Baseline before any metabolic-effect peptide.
- Cardiovascular assessment – EKG if age >40 or risk factors. Some peptides elevate heart rate.
- Allergy history & mast cell review – Have you had anaphylaxis? Chronic hives? Mast cell activation syndrome?
Absolute contraindications (don’t use peptides, period):
- Active cancer or personal/family melanoma history (especially Melanotan II)
- Uncontrolled diabetes
- Severe cardiovascular disease or recent MI
- Seizure disorder (melanotan II is contraindicated)
- Pregnancy or planning pregnancy
- Severe allergies or mast cell disorder
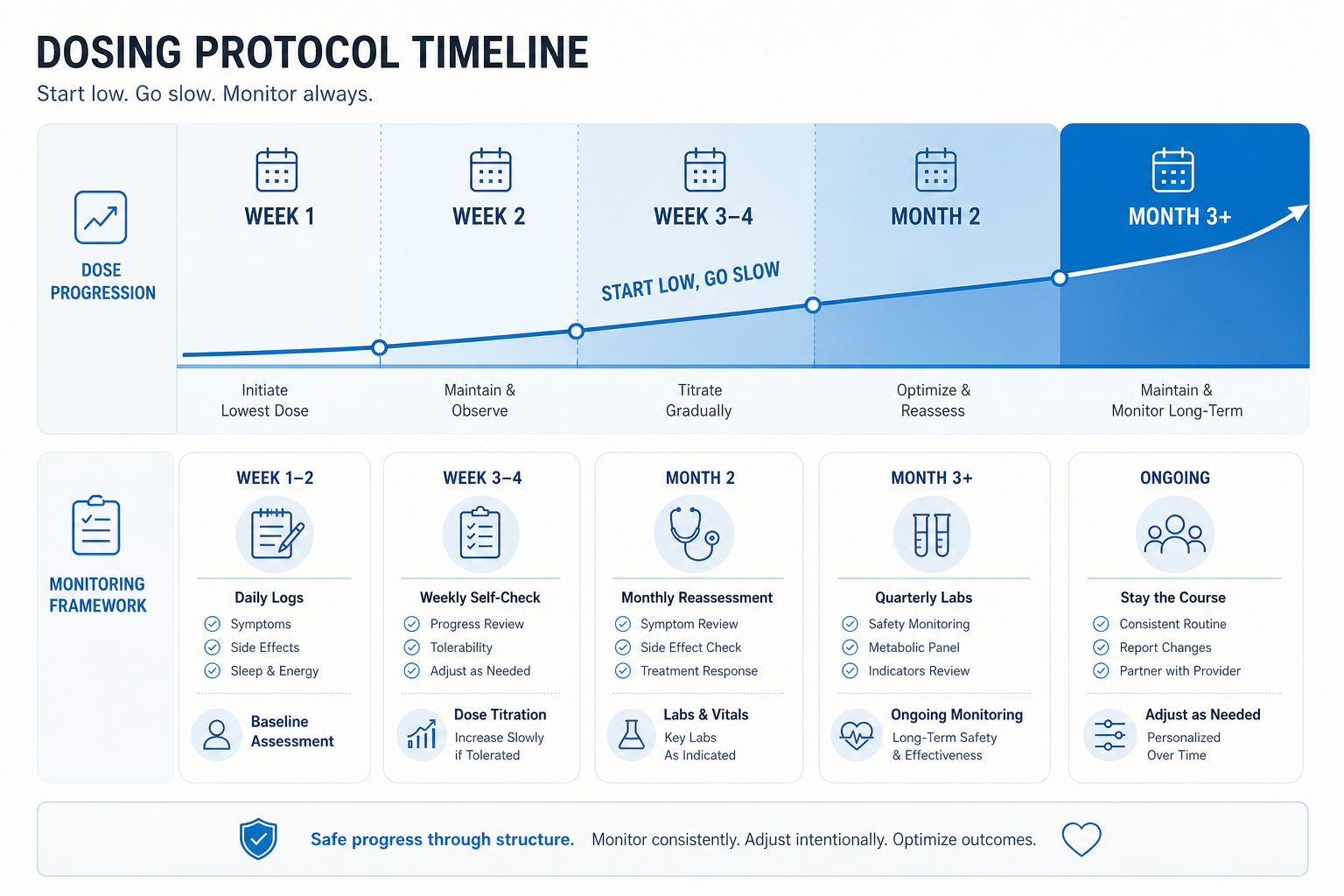
Step 2: Conservative Dosing
The phrase “start low, go slow” isn’t cute-it’s how you stay alive.
- Initial dose ≤25% of planned dose. Week 1-2, you’re testing tolerance, not chasing results.
- Precise measurement. Calibrated insulin syringes only (0.01 mL precision). Not hand measurement. Not eyeballing it. Document every single dose.
- Titration protocol. If no adverse effects after 2 weeks, increase to 50% of planned. After another 2 weeks, move to 75%. Reach full dose only after 4+ weeks with zero issues.
- Sterile technique. Autoclave-sterilized insulin needles, alcohol swabs, aseptic injection protocol, new needle every time.
- Site rotation. Inject a different site daily. Prevents lipohypertrophy and localized irritation.
Step 3: Daily Logging & Monitoring
For the first month, treat every injection like clinical data:
- Daily log: Injection time, dose, site, any symptoms. Energy? Mood? Sleep? Injection-site reaction? Systemic effects?
- Weekly self-check: Monitor for rash, swelling, joint pain, sleep changes, appetite changes.
- Monthly reassessment: Review the log for patterns. Any adverse effects accumulating?
- Quarterly labs (if ongoing): Repeat glucose, lipids, liver/kidney function. Catches late-onset effects.
Step 4: Emergency Preparedness
Have these available:
- Antihistamines (for allergic reactions)
- EpiPen (if anaphylaxis is a real risk)
- Emergency contact for a physician who understands peptides
Step 5: Clear Stop Criteria
Discontinue immediately if:
- Allergic reaction or signs of anaphylaxis
- Uncontrolled blood pressure or heart palpitations
- Severe nausea, vomiting, or abdominal pain
- Joint/muscle pain that worsens despite dose reduction
- Any neurological symptoms (seizures, severe headaches, confusion)
- Unexplained lab value changes (glucose, liver/kidney function)
Peptide Safety by Tier: What the Evidence Actually Says
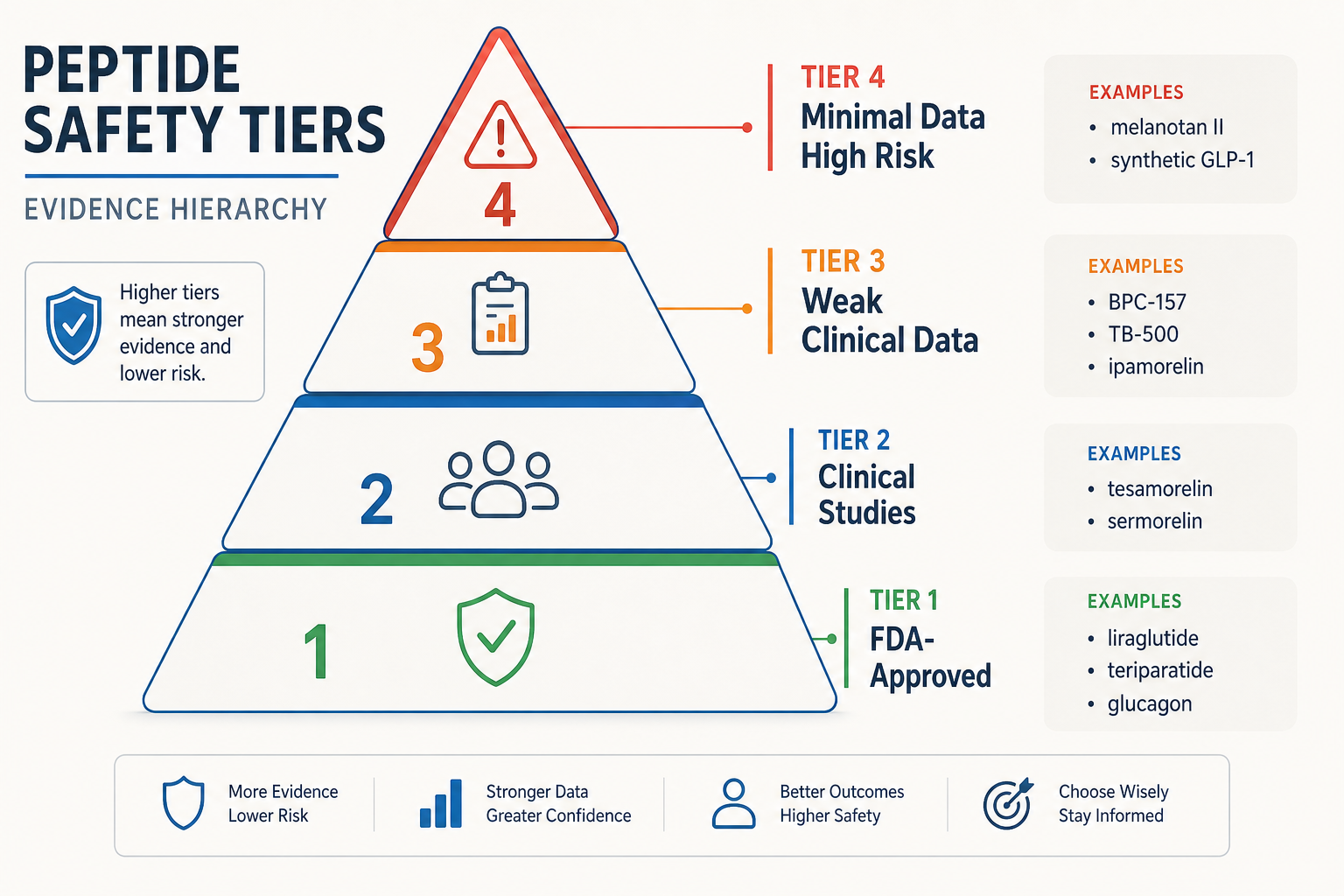
Not all peptides are created equal. Here’s what the clinical evidence actually shows:
Tier 1: FDA-Approved, Extensive Data
Liraglutide (Saxenda) – 20+ clinical trials. Adverse effects well-characterized. Nausea, vomiting, pancreatitis (rare), cardiovascular monitoring required.
Teriparatide (Forteo) – Long market history. Comprehensive safety profile. Injection-site reactions, dizziness, leg cramps documented.
Glucagon – Decades of emergency-medicine use. Adverse effects well-mapped.
Verdict: If you’re going to use peptides, start in this tier. Medical supervision still required. Baseline screening still needed.
Tier 2: Clinical Studies but Not FDA-Approved
Tesamorelin – HIV lipodystrophy trials show safety profile. Limited general population data. Moderate immunogenicity.
Sermorelin – Some human studies; generally safer than CJC-1295. Lower immunogenicity reported. Still experimental.
Verdict: Moderate evidence. Medical supervision recommended. More caution than Tier 1.
Tier 3: Mostly Preclinical, Weak Clinical Data
BPC-157 – Animal models suggest safety; minimal human trials. One case report of anaphylaxis-like reaction. Anticoagulant effects in rodents (risk in humans on blood thinners unknown).
TB-500 – Animal models only. Essentially no human clinical data. Immune modulation effects unclear.
Ipamorelin – Some human studies; weaker evidence base than sermorelin. Higher immunogenicity reports.
CJC-1295 – Higher immunogenicity reports than ipamorelin. Weak evidence overall. Lots of anecdotal reports; little clinical data.
Verdict: Use only with medical supervision. Serious gaps in human safety data. Treat as experimental.
Tier 4: Minimal/No Clinical Data, High Risk
Melanotan II – Significant adverse event reports. Seizures documented. Hypermelanization (darkening of skin/moles). Exacerbates melanoma risk (absolute contraindication if personal/family history).
Synthetic GLP-1 variants – If not FDA-approved formulations, safety is extrapolated from approved GLP-1s. That’s guessing. 381+ documented drug interactions with common medications.
Verdict: Avoid entirely unless under hospital-level medical oversight. The risk profile is steep.
Drug Interactions: The Ones That Matter
This isn’t a complete list-it’s the ones that land people in the ER:
GLP-1 agonists + insulin/sulfonylureas: Severe hypoglycemia. If you’re on insulin, your dose needs adjustment or elimination before starting GLP-1. This interaction is documented and serious.
GLP-1 agonists + warfarin/anticoagulants: INR levels shift. Monitoring required.
Peptides + antihistamines: May mask early signs of allergic reaction. Not ideal if you’re using peptides that carry immunogenicity risk.
GHRH peptides + thyroid hormones: Potential thyroid dysregulation. Baseline TSH required.
Melanotan II + any medication: Interaction data is basically nonexistent. Avoid combinations.
If you’re on any medication, audit it against known peptide interactions before first injection. A physician should do this, not you guessing from Reddit.
What Actually Reduces Risk
Medical supervision isn’t optional for systemic peptides. Community “doctors” don’t replace physicians.
Quality verification is foundational. Independent CoA validation + third-party testing catches contamination before it hits your bloodstream.
Baseline screening prevents ~70% of serious complications. Blood work + health history screening before first injection is non-negotiable.
Dosing discipline saves lives. Precise measurement + conservative dosing + titration > “standard dose.” Errors with GLP-1 require ER care.
Monitoring protocol catches adverse effects early when they’re reversible. Daily self-reporting + monthly labs.
Contraindication awareness. Know which peptides to avoid entirely. Melanotan II if you have seizure or melanoma history. GLP-1 if uncontrolled diabetes.
Stop criteria clarity. Have a plan to discontinue if adverse effects emerge. Don’t power through hoping they pass.
Chase the proof. Never the promise. That’s how peptides stay tools instead of becoming Russian roulette.
Frequently Asked Questions
What’s the difference between research-grade purity and sterility?
Purity measures the percentage of actual peptide present; sterility means the product is free of viable microorganisms. A 99% pure peptide can still harbor bacterial spores or endotoxins. Demand a CoA that shows both purity AND sterility testing (USP <71> or <797> certification).
Do I need a doctor’s approval to use peptides?
Medical supervision is non-negotiable for peptides with systemic effects (GLP-1 agonists, GHRH peptides, Melanotan II). A physician should review your baseline labs, contraindications, medication interactions, and dosing protocol. Community practitioners don’t replace physician oversight.
How much does independent peptide testing cost?
Third-party testing typically runs $200–500 per batch through accredited labs like Janoshik or Analytical Chemistry Labs. For high-risk peptides like GLP-1 or melanotan II, the cost is worth preventing contamination-related hospitalization.
What’s the safest peptide to start with?
Sermorelin and tesamorelin have the most clinical data outside of FDA-approved drugs. They show lower immunogenicity than CJC-1295 or ipamorelin. Still, baseline cardiovascular and allergy screening is mandatory before first injection.
If a vendor won’t share their CoA, should I buy from them?
No. Refusal to provide a certificate of analysis or allow third-party testing verification is a hard red flag. A legitimate vendor has nothing to hide and will provide documentation that traces back to an accredited testing lab.