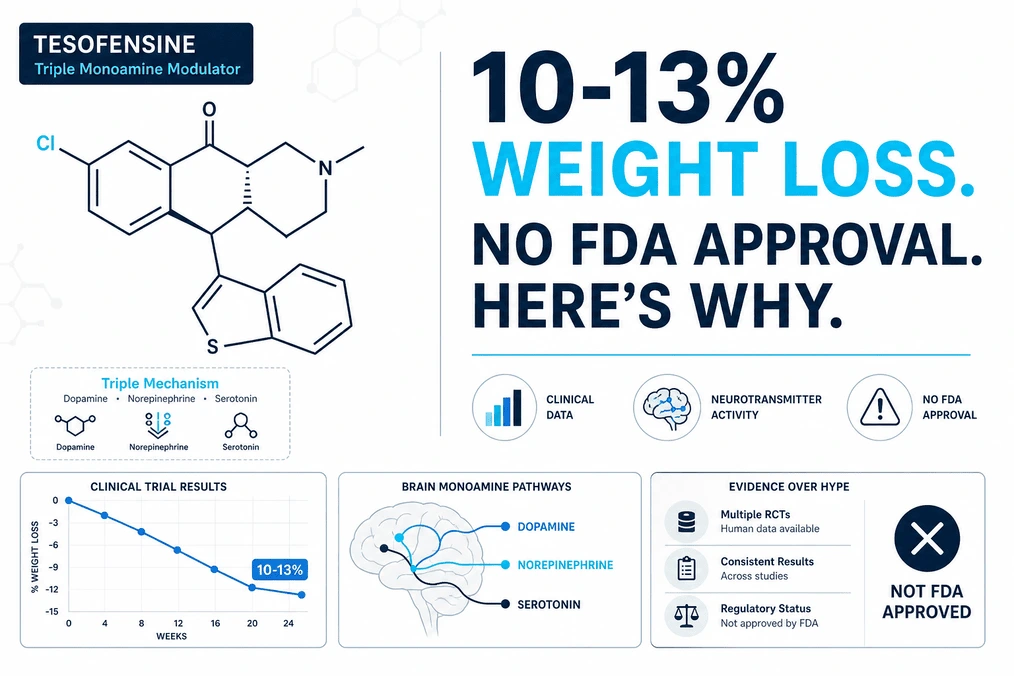
Tesofensine produced 10-13% weight loss in clinical trials-comparable to GLP-1 agonists. So why isn’t it FDA approved? We break down the science, the safety data, and whether it’s actually worth sourcing.
In 2008, researchers at NeuroSearch A/S noticed something unexpected. They were testing a compound called tesofensine as a potential Parkinson’s disease treatment. Patients in the trial weren’t getting better at Parkinson’s. But they were losing a lot of weight.
The compound suppressed appetite so reliably that within 24 weeks, patients were down 10-13% of their body weight. For context, that’s in the ballpark of modern blockbuster obesity drugs like semaglutide (Ozempic, Wegovy). Tesofensine worked through a completely different mechanism-targeting monoamine reuptake in the brain instead of gut hormones.
By all reasonable measures, this should have become a landmark weight-loss drug. It didn’t. Tesofensine is not FDA approved. It’s not available by prescription anywhere in the U.S. You can’t get it at a pharmacy. What you can do is source it from research chemical vendors for $100-400 per month, fully unregulated and without medical oversight.
Why? That’s the paradox we’re breaking down today.
TL;DR
Tesofensine is a triple monoamine reuptake inhibitor that produced 10-13% weight loss in Phase II trials-comparable to GLP-1 agonists but through a different brain mechanism. It’s not FDA approved because the developer went bankrupt, cardiovascular safety concerns (7-9 bpm heart rate increase) made the FDA cautious, and no sponsor funded Phase III trials.
Real clinical data stops at 24 weeks; long-term safety is unknown. Community reports suggest ~40-50% high responders who lose 3-7 lbs/week, with most users cycling 8-12 weeks on, 4-8 weeks off, to avoid unknown risks. If considering it, understand you’re using a research chemical with no quality control and no medical supervision standard-cardiac monitoring before starting is wise.
The Paradox: Strong Science, No Approval
It doesn’t make intuitive sense. A compound produces reproducible, clinically significant weight loss in a double-blind, placebo-controlled trial published in The Lancet. The mechanism is understood. The side effect profile is manageable in the short term. And yet:
It’s been 18 years since that trial. Tesofensine has never been approved for obesity.
Here’s what actually happened:
NeuroSearch went bankrupt in 2011. Development halted before Phase III trials could finish. At that point, ownership transferred to Saniona A/B, the current rights holder. But Saniona pivoted toward rare diseases (specifically Prader-Willi syndrome) rather than general obesity. Building out an obesity indication requires expensive Phase III trials (now including mandatory cardiovascular outcome trials per FDA guidance). No one has bankrolled that.
The FDA’s position is cautious. Tesofensine increases resting heart rate by 7-9 beats per minute-a sympathomimetic effect of norepinephrine reuptake inhibition. Post-sibutramine (an older weight-loss drug pulled from market for cardiovascular risk), the FDA became skeptical of sympathomimetic compounds. They want a full cardiovascular outcome trial before even considering approval. That trial has never been done.
Translation: The compound works. The science is solid. The economics don’t add up, and the regulatory environment is hostile.
This is why tesofensine lives in a legal gray area-neither approved nor scheduled, available through unregulated research chemical vendors, self-dosed by informed biohackers and peptide researchers willing to accept unknown long-term risks for documented short-term efficacy.
How Tesofensine Works: Triple Monoamine Mechanism
Tesofensine blocks the reuptake of three neurotransmitters in the brain: serotonin, norepinephrine, and dopamine. This is fundamentally different from how GLP-1 agonists work, and it’s why the compound offers a genuinely novel angle on weight loss.
Serotonin reuptake inhibition → satiety signaling. Your brain interprets nutrient availability differently; you feel full sooner.
Norepinephrine reuptake inhibition → mild sympathomimetic effect. Increased alertness, slight metabolic boost, and the heart rate elevation that worries regulators.
Dopamine reuptake inhibition → reward/craving suppression. Food cravings diminish; the motivational drive to eat decreases. This is the unique lever GLP-1s don’t have.
A 2010 mechanistic study published in the International Journal of Obesity placed users in a respiratory chamber and measured energy expenditure directly. Tesofensine didn’t boost metabolism. It suppressed appetite-specifically, a 24% reduction in energy intake. Resting metabolic rate stayed the same. The weight loss came entirely from eating less, not from burning more.
This distinction matters. Unlike stimulant-based weight loss (phentermine), tesofensine isn’t forcing your metabolism to work harder. Unlike GLP-1s, it’s not signaling the gut. It’s directly modulating the brain’s appetite control center. Recent preclinical work (2024) identified the exact circuit: tesofensine silences GABAergic neurons in the lateral hypothalamus, the brain region that normally suppresses appetite suppression. Kill that brake, and appetite suppression sticks.
For biohackers, this opens a genuine question: would tesofensine work for people who don’t respond to GLP-1s? The mechanisms are different enough that synergy is plausible. But no one’s tested it. The clinical evidence stops at single-drug trials.
The Clinical Evidence: What the Trials Actually Show
The landmark study is the TIPO-1 trial, published in The Lancet in 2008. This is where the 10-13% figure comes from, and understanding what it actually means is critical before considering sourcing.
Trial design: 203 overweight and obese adults, randomized double-blind to placebo or tesofensine at one of three doses (0.25 mg, 0.5 mg, 1.0 mg daily). 24 weeks. Measured weight loss, body composition, quality of life.
Results at the 0.5 mg dose (the most studied):
- Mean weight loss: 11.3% vs. 2.2% placebo (a 9% absolute difference)
- 87% achieved ≥5% weight loss
- Weight loss accrued steadily through the 24-week period (not front-loaded)
- Body composition favored lean mass preservation (higher protein loss would be worse)
For comparison: Semaglutide (Ozempic) in obesity trials produces 10-22% weight loss at the 2.4 mg dose, so tesofensine’s 11.3% puts it in the effective range, not the blockbuster range.
The critical caveat: Trial length was 24 weeks. No clinical data exists beyond that. We don’t know if:
- Weight loss continues past 24 weeks (tolerance might develop)
- Weight rebounds when discontinuing (how much? how fast?)
- Side effects persist or worsen with extended use
- Lean mass preservation holds up long-term
This is the gap that makes community cycling strategies (8-12 weeks on, 4-8 weeks off) a conservative hedge. Users are essentially saying: “We know it works for 24 weeks. We don’t know about month 12. Let’s not stay on it indefinitely.”
What Users Actually Report: Community Sentiment
Reddit threads on tesofensine are remarkably consistent. The r/Tesofensine_ subreddit and discussion threads on r/Peptides and r/Nootropics paint a picture of real-world efficacy that roughly aligns with trial data, with important nuances.
Efficacy distribution: About 40-50% of users report complete appetite suppression (high responders), 30-40% report moderate appetite reduction, and 10-20% report minimal effect. This distribution roughly mirrors trial data-not everyone responds equally.
Weight loss velocity: High responders report 3-7 lbs per week at the 0.5 mg dose, but this assumes dietary compliance. The compound suppresses appetite; it doesn’t guarantee you’ll eat less if you override the signal with willpower or habit.
“Day 4 on 0.25 mg and I’m genuinely not hungry. I have to remind myself to eat. It’s weird in a good way.” – r/Tesofensine_
“Three weeks in. Down 8 lbs. The appetite suppression is real, but dry mouth is brutal. I’m going through a liter of water a day.” – r/Peptides
“Week 6, 0.5 mg. I’m a high responder. Down 12 lbs, not hungry, sleeping fine. But my resting HR went from 62 to 71. I’m getting an EKG to make sure nothing weird is happening.” – r/Nootropics
Cycling patterns: Most experienced users report practicing 8-12 weeks on, 4-8 weeks off. The rationale: we have 24-week safety data; we don’t have 6-month or 12-month data. Cycling is a self-imposed safety limit.
Tolerance: Users report sustained appetite suppression through 12 weeks (matching trial data), but anecdotal reports of tolerance emerging around week 16-20 exist. Again, no clinical data confirms this.
Side effects in the wild: Dry mouth (60-70% of users, most tolerable), insomnia (40-50%, worse if dosed in evening), elevated heart rate (50-60% notice it). Most report side effects are manageable but real.
The community is notably aware of unknown risks. These aren’t desperate people ignoring safety-they’re informed early adopters willing to accept short-term known risks for a chance at effective weight loss, with conservative hedging strategies (cycling, cardiac monitoring) in place.
Safety Profile: What You Need to Know
The short-term safety data from the TIPO-1 trial is reasonably clean. The long-term safety is genuinely unknown.
Most common side effects in trials:
- Dry mouth: 30-44% (annoying but tolerable; usually decreases over time)
- Insomnia: 21-35% (worse with evening dosing; morning dosing helps)
- Nausea: 10-20% (usually mild and transient)
- Headache: 10-15%
- Elevated heart rate: 7-9 bpm increase (reversible on discontinuation)
The cardiovascular signal: This is the regulatory sticking point. Tesofensine consistently increases resting heart rate by 7-9 beats per minute. This is sympathomimetic-it’s the norepinephrine reuptake inhibition at work. In short-term trials, this was not associated with other adverse events, but it’s the reason the FDA wants a full cardiovascular outcome trial before approval. They want to know: does this heart rate elevation translate to real cardiac events (MI, stroke, arrhythmia) in a large population over years of use?
The honest answer: nobody knows. The compound has not been studied long enough, in a large enough population, with adequate cardiovascular monitoring, to rule out risk.
For someone considering tesofensine, pre-baseline cardiac assessment is reasonable: resting heart rate, blood pressure, and possibly an EKG (especially if any cardiovascular risk factors exist). During use, monitoring HR and BP regularly is prudent. This is self-care in the absence of clinical oversight-not perfect, but better than flying blind.
Drug-drug interactions: Tesofensine is a monoamine reuptake inhibitor. Combining it with SSRIs, SNRIs, MAOIs, or stimulants could theoretically trigger serotonin syndrome. This has not been clinically tested. Anyone on psychiatric medications should be very cautious and ideally consult a knowledgeable clinician before considering tesofensine.
Special populations: Tesofensine has not been studied in pregnant individuals, people with cardiac disease, people with psychiatric disease, elderly individuals, or people on multiple medications. If any of those categories apply, the risk-benefit calculation shifts significantly toward “don’t use.”
Tesofensine vs. GLP-1 Agonists: Mechanism Matters
This is where tesofensine’s fundamental difference becomes strategically relevant.
| Attribute | Tesofensine | GLP-1 Agonists (Semaglutide, Tirzepatide) |
|---|---|---|
| Mechanism | Brain monoamine reuptake inhibition (appetite suppression) | Gut hormone signaling (GLP-1 + GIP receptors) |
| Route | Oral capsule daily | Subcutaneous injection weekly |
| Efficacy | 10-13% weight loss (24 weeks) | 10-22% weight loss (68 weeks, dose-dependent) |
| Lean mass preservation | Trial signal suggests favorable | Mixed; some lean mass loss reported |
| GI side effects | Dry mouth, insomnia, HR elevation | Nausea, vomiting, GI distress common |
| Long-term data | None beyond 24 weeks | 68+ weeks in Phase III trials |
| FDA approval | Not approved | Approved for obesity |
| Cost | $100-400/month (unregulated vendors) | $1,000-1,500/month (insurance may cover) |
| Non-responder rate | ~10-20% report minimal effect | ~15-20% report minimal effect |
The strategic angle: If you respond well to GLP-1s, there’s no compelling reason to switch. GLP-1 efficacy is proven and approved. If you don’t respond well to GLP-1s (or can’t tolerate the GI side effects), tesofensine represents a genuinely different mechanism that might work. But that’s speculation-no head-to-head comparative trial exists.
The oral dosing and lean mass preservation profile are theoretical advantages. The lack of FDA approval and long-term safety data are material disadvantages.
How to Source Tesofensine: Legal Gray Area
Tesofensine is not scheduled as a controlled substance. It’s not explicitly illegal to purchase or possess. But it’s also not FDA-approved for any indication. This creates a legal gray area.
The market: Unregulated research chemical vendors sell tesofensine for ~$100-400 per month, depending on dose and vendor. Purity is unverified; most users don’t test. Some compounding pharmacies may synthesize it (legal gray area). Some users source Tesomet (tesofensine + metoprolol combination, approved for rare disease trials in some jurisdictions) from international sources.
Quality control: There isn’t any. You’re purchasing from vendors with financial incentive to misrepresent purity. No independent testing standard exists. Users in the community sometimes report testing via third-party labs, but that’s self-funded and not widespread.
Legal enforcement reality: There have been no prosecutions of individual users for tesofensine possession in the U.S. The compound is too niche and of low regulatory priority. But “legal gray area” is not the same as “legal”-that status could change if the compound gains mainstream attention.
Risk acceptance: Anyone sourcing tesofensine is making a deliberate choice to use an unapproved compound without medical supervision. This is not inherently irrational (the efficacy data is real), but it’s a choice to accept regulatory, quality-control, and safety risks that approved medications don’t carry.
Read our guide before you buy tesofensine online.
The Bottom Line: Decision Framework
Here’s how to think about tesofensine if you’re considering it:
You should consider tesofensine if:
- You’ve tried GLP-1 agonists and either didn’t respond or couldn’t tolerate GI side effects
- You’ve tried other weight-loss approaches (diet, exercise, other medications) and hit a plateau
- You understand and accept that long-term safety is unknown
- You’re willing to monitor your cardiovascular status (resting HR, blood pressure, ideally baseline EKG)
- You’re capable of sourcing reliably from a vendor and potentially testing purity
- You’re comfortable with regulatory gray area and potential legal ambiguity
You should not consider tesofensine if:
- You have any history of cardiac disease, arrhythmia, or hypertension
- You’re on SSRIs, SNRIs, MAOIs, or stimulant medications
- You’re pregnant, breastfeeding, or planning to become pregnant
- You’re unwilling or unable to monitor cardiovascular markers
- You need FDA-approved, regulated compounds with long-term safety data
If you do go the route of tesofensine:
- Get a baseline resting heart rate, blood pressure, and ideally an EKG
- Dose conservatively (0.25-0.5 mg daily, morning dosing to avoid insomnia)
- Monitor resting HR and BP weekly; escalate if HR rises more than 10-12 bpm
- Cycle: 8-12 weeks on, 4-8 weeks off (conservative approach to unknown long-term effects)
- Stay hydrated (dry mouth is real) and maintain basic nutrition
- Consider consulting a peptide-friendly clinician or your doctor, even if sourcing is self-directed
Tesofensine is genuinely effective at suppressing appetite and producing weight loss in the short term. It’s also genuinely understudied for long-term safety. The research bias matters.
Frequently Asked Questions
Is tesofensine actually approved for weight loss?
No. Tesofensine was never approved by the FDA for obesity. It passed Phase II clinical trials (producing 10-13% weight loss), but development stalled when the developer went bankrupt. The FDA subsequently became cautious due to cardiovascular safety signals. A rare disease trial is ongoing for Prader-Willi syndrome, but no obesity indication is in the FDA pipeline.
How much weight loss does tesofensine actually produce?
In Phase II trials, tesofensine at 0.5 mg produced 11.3% mean weight loss over 24 weeks vs. 2.2% for placebo-a 9% difference that’s comparable to modern GLP-1 agonists. The landmark TIPO-1 trial showed 87% of patients achieved at least 5% weight loss. Community reports suggest 3-7 lbs/week depending on diet adherence, but long-term data beyond 24 weeks doesn’t exist.
What are the main side effects?
Dry mouth (30-44% in trials), insomnia (21-35%), and nausea (10-20%) are most common and usually manageable. The critical concern is heart rate elevation: tesofensine increases resting heart rate by 7-9 beats per minute, a sympathomimetic effect that sparked FDA regulatory caution. This is reversible when discontinuing but represents a real safety signal that requires monitoring.
Is it safe to use long-term?
Unknown. Clinical trial data only extends to 24 weeks. No safety data exists beyond that timeframe. This is why most users in the research community practice cycling (8-12 weeks on, 4-8 weeks off) rather than continuous use-they’re choosing a conservative approach to an unknown risk. If considering tesofensine, cardiac monitoring (resting HR, blood pressure, potentially an EKG) before starting is prudent.
How is tesofensine different from GLP-1 agonists like semaglutide?
Tesofensine suppresses appetite via the brain (monoamine reuptake); GLP-1s work via the gut (hormone signaling). This means tesofensine may preserve lean muscle better (trial signal suggests this), causes fewer GI side effects, and is oral rather than injected. It might also work for people who don’t respond to GLP-1s. However, no head-to-head trial comparing them exists, so direct efficacy comparison is speculation. The cardiovascular safety profile is also less established than GLP-1s.